
Compiled by the clinical team at Home Dental Centre|Last updated: July 2026
Reader Notice
- This article provides general dental health information only and cannot replace a clinical diagnosis by a dentist or doctor.
- If you experience difficulty breathing, difficulty swallowing, rapidly spreading facial or neck swelling, persistent high fever, severe trauma or heavy bleeding, go to a hospital Accident & Emergency department immediately.
- Arrangements for government dental street sessions, hospital A&E and other public healthcare services may change; always refer to the latest official announcements.
Introduction: what makes toothache truly stressful is often not the pain — it's not knowing what to do next
You wake at 2am in sudden pain — should you take a painkiller first, or find a dentist straight away? Your face starts swelling on a Sunday — should you go to a hospital A&E, or wait until Monday? A filling falls out but nothing hurts — is it safe to watch and wait for a few days? Your child falls and knocks a tooth — there isn't much blood, so do you really need to see someone immediately?
Most people in Hong Kong rarely think about dental emergencies until the day they have one. Then the searching begins. Some search "toothache what to do", some search "will A&E treat teeth", some search "government dental street sessions", and some search "Sunday dentist". The more you read, the less certain you feel.
The problem is not a lack of information — it's that the information is fragmented. Some articles are more than a decade old; some describe healthcare systems in other countries; some are just forum comments; and some widely repeated claims simply no longer apply to Hong Kong today.
For example, many people still believe you must queue outside a government dental clinic before dawn; others assume every toothache belongs in a hospital A&E; and some believe that as long as painkillers work, the tooth must be fine. None of these beliefs is surprising. Most people encounter a genuine dental emergency only a few times in their lives, so their judgement is built from friends' stories, family hearsay and scattered online posts.
This article is not meant to alarm you, nor to tell you which clinic to visit, nor to push you toward any treatment. Our only goal is to lay out — as simply and objectively as we can — the twelve things Hong Kong people most often misunderstand about dental emergencies, and most often waste time on as a result.
If you're only reading this out of curiosity today, we hope you won't need it for a very long time. But if one day you, your family, or your child faces a real dental emergency, we hope this article leaves you a little less anxious, a little less unsure, and much clearer about what to do next.
"Dental emergency", "emergency dentist", "urgent dental care" — different search terms, same question
People search "Hong Kong dental emergency", "emergency dental care", "urgent toothache", "emergency dentist", "same-day dentist" or "Sunday dentist" — but what they really want to know is rarely which term is correct. It is: what should I do right now? Do I need a hospital A&E? How do government dental street sessions actually work? Can this wait, or should a dentist examine it as soon as possible? This article walks through the most common misunderstandings and general guidance based on how things currently work in Hong Kong.
The One-Minute Summary
If you're searching this article because you're in pain right now, you may not have time to read it all. Remember these five things first.
- Painkillers can temporarily reduce pain, but they cannot treat the underlying problem in the tooth.
- Ordinary toothache does not usually require a hospital A&E — but if you already have difficulty breathing, difficulty swallowing, rapidly spreading facial swelling or severe trauma, go to A&E immediately.
- Government dental street sessions now use online registration and a computer ballot — you can no longer simply queue at the clinic to be seen.
- Many teeth with cracks, abscesses or inflamed nerves can still be saved with appropriate treatment — extraction is not always necessary.
- If you're unsure whether your situation counts as an emergency, a prompt clinical assessment by a dentist usually finds the real cause faster than endless searching.
Three Familiar Hong Kong Scenarios
Scenario 1: Woken at 2am by toothache
The most common response is to take a painkiller and hope to last until morning. If the pain clearly improves and there is no swelling or fever, you may not need an A&E in the middle of the night. But if the pain keeps you from sleeping, the painkillers wear off faster and faster, or your gums begin to swell, you should not simply keep observing on medication alone.
Scenario 2: A wisdom tooth flares up on a Sunday
What makes Sundays stressful is not knowing where to go — A&E, a government session, or waiting until Monday. If it's localised gum pain and swelling, arrange a dental assessment as soon as possible. If you already have difficulty opening your mouth, pain on swallowing, fever, or facial swelling that is getting worse, treat the situation with far more caution.
Scenario 3: A child falls and injures a front tooth
Many parents judge by how much blood there is. But dental trauma is not only about bleeding. Even when a tooth doesn't look loose, the root, the supporting tissues, or a developing permanent tooth underneath may be affected. After any dental injury, children should generally be examined by a dentist promptly.
Thing 1: "It's just toothache — surely it can wait until tomorrow?"
This may be the single most common thought in Hong Kong. After all, most toothaches don't appear suddenly — they start as mild sensitivity, become discomfort when eating, and gradually turn into persistent pain.
Most of us have taken a painkiller, felt a little better the next day, and naturally concluded: "Let's wait one more day and see." There is nothing wrong with hoping things improve on their own — nobody wants to take leave, change plans, or spend a day seeking care.
But teeth are different from most tissues in the body: they have almost no capacity to heal themselves. If the pain is caused by decay, an inflamed nerve, a root infection, a cracked tooth or an acutely infected wisdom tooth, the underlying problem usually remains even when the pain temporarily eases.
Brief sensitivity to hot or cold is not necessarily an emergency. But if pain has lasted for several hours or more, is affecting your sleep, if painkillers are wearing off faster, or if gum swelling, an abscess or facial swelling appears, waiting is generally not advisable.
In one line
- Pain relief can wait a few hours; the real cause should not be left waiting indefinitely.
Thing 2: "Severe toothache means I should go to a hospital A&E, right?"
For many people facing severe tooth pain for the first time, the hospital Accident & Emergency department is the first place that comes to mind. It's an understandable reflex — the word "emergency" makes us think any sudden, intensely painful problem belongs there.
But dental emergencies and general medical emergencies are not the same thing. A hospital A&E's primary role is to prioritise conditions that may be life-threatening or rapidly deteriorating — severe trauma, heavy bleeding, infections affecting the airway. Patients are triaged by severity.
For ordinary toothache — however intense — an A&E usually cannot provide definitive dental treatment. The situations that genuinely require an immediate A&E visit are those where a dental problem has begun to affect the whole body: rapidly spreading facial or neck swelling, difficulty breathing, difficulty swallowing, persistent high fever, major facial trauma or heavy bleeding.
If the problem remains centred on the tooth itself — severe pain from decay, an inflamed nerve, an abscess, an acutely infected wisdom tooth, a fractured tooth, or a lost crown or filling — it usually still needs a dentist's examination, with dental X-rays where necessary, to identify the true cause.
In one line
- Most toothaches need a dentist's diagnosis and treatment; go straight to a hospital A&E if you have difficulty breathing or swallowing, severe infection or major trauma.
Thing 3: "Government dental street sessions — can't I just turn up and be seen?"
Many people searching for "government emergency dental" are really looking for the government's dental street sessions (GP sessions). Some believe that arriving early enough guarantees same-day treatment; others assume any toothache can be handled there.
Currently, government dental street sessions allocate places by online registration and computer ballot — you can no longer simply queue at the clinic to be seen. Successful applicants attend a designated clinic at a designated date and time.
The service also has a clearly defined scope: it provides limited emergency dental care — chiefly management of acute pain and extractions — not general dentistry. It does not include scaling, routine fillings, crowns, dentures or other regular treatment.
So if what you actually need is to save the tooth — root canal treatment, periodontal care, re-cementing a crown or bridge, or other more complex work — you will still likely need a full dental examination to determine the most suitable treatment plan.
In one line
- Government dental street sessions are a valuable public service with a defined scope, quota system and registration process — check the latest official arrangements before you go, and you'll avoid a wasted trip.
Thing 4: "Toothache must mean a cavity"
"It must be a cavity" is many people's first assumption. Decay is indeed one of the most common causes of toothache — but far from the only one.
The same kind of pain can have entirely different causes. An acutely infected wisdom tooth can make the whole lower jaw, the ear, even the throat hurt. A cracked tooth may feel completely normal until you bite at exactly the wrong angle and get a jolt of sharp pain. Gum (periodontal) disease can cause swelling and aching from inflamed gum and supporting tissue.
Some patients are certain a particular tooth is the culprit — only for the examination to reveal that the real problem lies in the tooth next door. Teeth can produce "referred pain": the place that hurts is not always the place with the problem.
That is why, beyond looking in your mouth, a dentist will often take dental X-rays, test the nerve's vitality, and perform other clinical checks to narrow down the true cause step by step.
In one line
- Cracked teeth, wisdom teeth and gum disease can all cause toothache — the cause needs to be confirmed clinically, not assumed.
Thing 5: "The pain has stopped — so the problem is gone"
When pain fades, it's natural to relax and assume the tooth has recovered. Sometimes that's true. But sometimes, the disappearance of pain means something quite different.
When the nerve inside a tooth is severely inflamed or infected, there can be a stage where the nerve begins to die — and as it dies, the pain may fade or vanish. The infection, however, may continue to spread quietly toward the root tip and surrounding bone.
Some patients only discover this when swelling, an abscess or pain on biting appears weeks or months later — by which point the treatment required may be more involved than it would have been at the start.
Pain is a signal, not a diagnosis. Its absence is not proof that the disease has gone.
In one line
- Pain that suddenly disappears does not always mean recovery — it can mean the nerve is already affected.
Thing 6: "A cracked tooth always has to be extracted"
Hearing the word "cracked" makes many patients assume the tooth is beyond saving. In reality, whether a cracked tooth can be kept depends heavily on where the crack is and how deep it goes.
Shallow surface craze lines are common and often need no treatment at all. A crack limited to the crown of the tooth may be repairable with a filling, an onlay or a crown. If the crack reaches the nerve, root canal treatment followed by a protective crown may still save the tooth.
Only when a crack extends below the gum or splits the root is extraction usually unavoidable. That's why a dentist will assess the crack's position, depth and the tooth's overall condition — sometimes with X-rays and bite tests — before recommending anything.
In one line
- Not every cracked tooth needs extraction — it depends on the location and depth of the crack.
Thing 7: "My crown fell off — what should I do?"
A crown, filling, bridge or veneer can occasionally come off — sometimes with no pain at all, which tempts people to wait, or to try glueing it back themselves.
Two things matter here. First, keep the item safe — bring it with you, because in some cases it can be cleaned and re-cemented. Second, do not use household glue or adhesive of any kind to reattach it: these materials are not designed for the mouth, can damage the tooth, and often make proper re-cementing impossible.
Even without pain, the exposed tooth underneath has lost its protection and is more vulnerable to decay, fracture and sensitivity. Prompt assessment lets the dentist decide whether the original restoration can be reused or a new one is needed.
In one line
- Keep whatever fell off, never glue it back yourself, and see a dentist as soon as possible.
Thing 8: "My wisdom tooth is infected — pull it out today"
When a wisdom tooth flares up, many patients ask to have it removed on the spot: "It'll have to come out eventually — why not today?" The reality is often less simple.
Wisdom tooth infections are frequently linked to partial eruption: a hard-to-clean pocket forms between gum and tooth, trapping food debris and bacteria and causing localised inflammation, pain and swelling.
Some patients also develop difficulty opening the mouth, pain on swallowing, or mild facial swelling. A dentist will typically assess the severity of infection, mouth opening, tooth position and your overall health before deciding whether immediate extraction is appropriate.
In some cases, controlling the infection first and scheduling the extraction afterwards is safer and makes the surgery more straightforward. For wisdom teeth that flare up repeatedly, the dentist may still recommend removal once things have settled — precisely to prevent the next episode.
In one line
- An infected wisdom tooth doesn't always need immediate extraction — control the infection first, then let clinical assessment decide the timing.
Thing 9: "Emergency treatment is just about stopping the pain, isn't it?"
A common assumption about emergency dentistry: "Stop the pain first, deal with the rest later." It's an understandable view — pain is the most immediate experience, so no pain feels like problem solved.
But the real point of an emergency dental visit is usually not pain relief in itself — it's identifying what's causing the pain. Severe toothache alone could be an inflamed nerve, a root infection, a cracked tooth, or simply a lost filling leaving the tooth unprotected.
That's why, at an emergency visit, the dentist will typically take a history, examine the teeth and mouth, arrange dental X-rays where needed, and only then determine the actual diagnosis — rather than deciding upfront whether to fill, root-treat or extract.
Many patients receive meaningful initial treatment at that first visit: infection control, drainage of an abscess, re-cementing a crown, a temporary restoration, or the first stage of root canal treatment.
In one line
- The goal of emergency dental care is not just pain relief — it's finding the cause, controlling the problem, and saving the tooth wherever possible.
Thing 10: "The tooth that hurts is the tooth with the problem"
"Doctor, I'm certain it's this one." Yet it is not unusual, clinically, for the real culprit to be a different tooth from the one the patient feels.
One reason is referred pain: an affected tooth can send pain to neighbouring teeth, the upper or lower jaw, even the ear, temple or cheek.
A lower molar with an inflamed nerve, for example, can convince a patient the pain is coming from an upper tooth; others feel a whole side of the mouth aching without being able to point to any single tooth.
This is why a dentist won't examine only the tooth you point to — they'll check the neighbouring teeth one by one and, where needed, use X-rays, nerve vitality tests and bite tests to locate the true source.
In one line
- The spot that hurts most is not necessarily the problem tooth — accurate diagnosis requires clinical examination.
Thing 11: "Emergency dental care must be expensive"
Many people endure pain not because they can bear it, but because they're worried about cost. "Will an emergency dentist be expensive?" "Will they insist on lots of treatment?" These are very common concerns.
Different clinics structure fees differently — there is no single standard. Some charge separately for consultation, X-rays, medication and treatment; some treatments depend on the tooth's condition, complexity and time required.
That's why it is entirely reasonable to understand the diagnosis, the treatment options and the associated fees before agreeing to anything. After an examination, most dentists will explain the current situation, the available options and their approximate costs.
On the other hand, many people delay care out of cost anxiety, hoping the problem resolves itself. Unfortunately, some dental problems that are left to progress end up requiring treatment considerably more complex — and more costly — than what would have been needed at the start.
In one line
- Rather than guessing at costs, find out the actual diagnosis first — then decide based on the treatment plan and the fees explained to you.
Thing 12: "If I search online, I'll figure out what's wrong"
Faced with any health problem today, most of us reach for our phones first. Online health information genuinely helps — it teaches basic concepts and flags situations that need urgent attention.
The catch is that many dental conditions share very similar symptoms. The same "toothache" could be decay, a cracked tooth, an inflamed nerve, gum disease, an acutely infected wisdom tooth, a loose crown — or pain that doesn't originate from a tooth at all.
Search by symptoms alone and you'll find plenty of answers that all "sound exactly like me". Much online content also comes from other countries, whose healthcare systems, referral routes and treatment arrangements differ from Hong Kong's.
Treating online information as a starting reference is sensible. But actual diagnosis and treatment still require a dentist's clinical examination — supported by X-rays where needed — of your specific situation.
In one line
- Online information helps you understand the landscape, but it cannot replace clinical examination — a real diagnosis is made for the individual patient, not the search term.
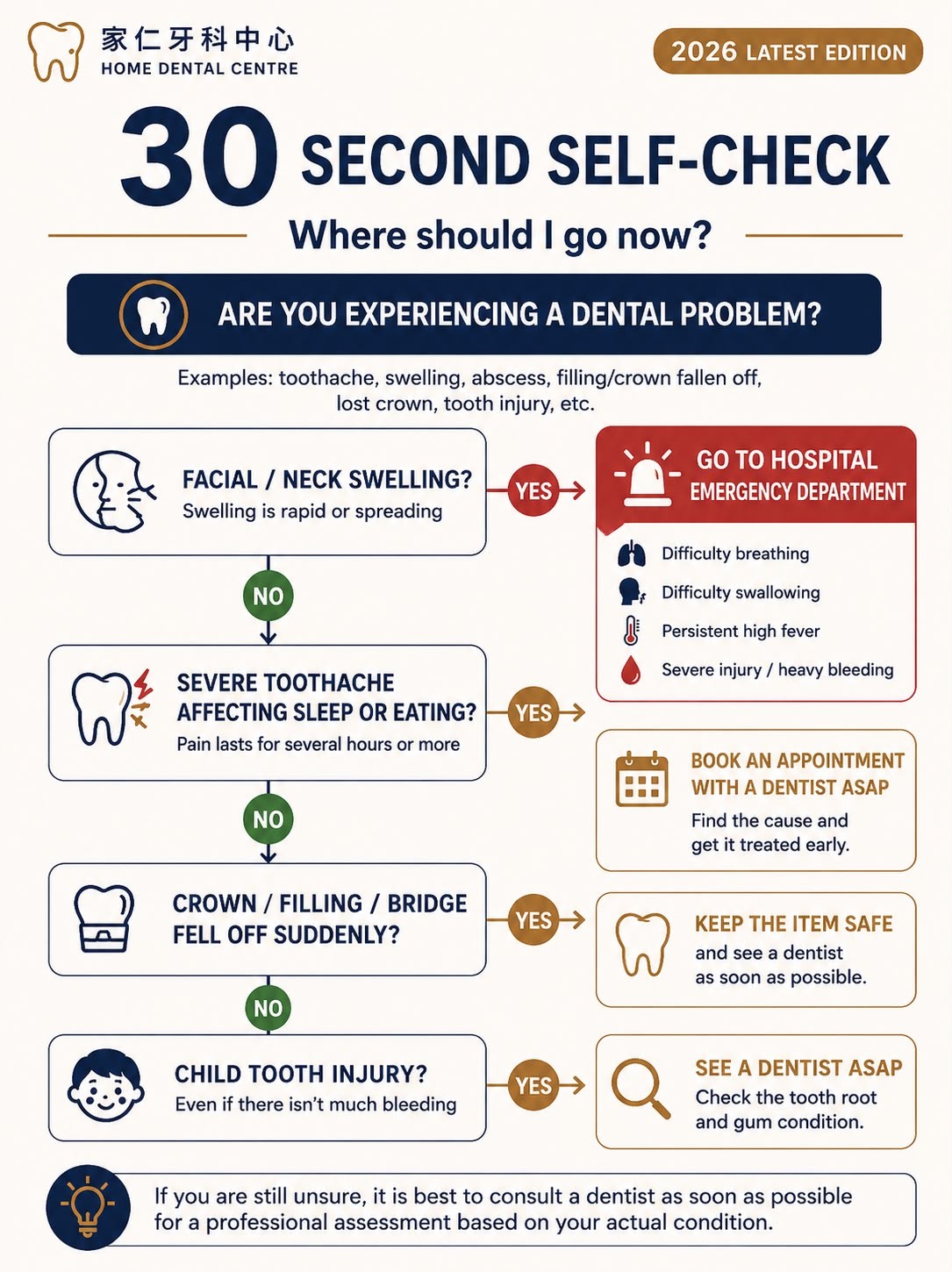
The 30-Second Self-Check: what should I do right now?
By this point, what you probably want most is not more dental knowledge but a direct answer: "If this is me right now, what's my next step?" Every patient's situation differs, but the following serves as general guidance.
| Situation | General guidance |
|---|---|
| Brief hot/cold sensitivity that settles quickly once the trigger is removed | Not necessarily an emergency — arrange a routine dental check-up. |
| Toothache lasting several hours or more, affecting sleep, eating or work | Don't keep waiting — have a dentist assess it as soon as possible. |
| Gum swelling, an abscess, or the face starting to swell | Seek dental assessment promptly; if swelling spreads rapidly with high fever, difficulty breathing or swallowing, go to a hospital A&E immediately. |
| Tooth injured in a fall, sport or traffic accident | Even with little bleeding or no obvious looseness, see a dentist promptly. |
| A filling, crown, bridge or veneer suddenly falls off | Keep the item, don't glue it back yourself, and arrange a dental examination. |
Five Decisions People Most Often Regret
Hoping it will "get better by itself tomorrow"
Work is busy, the kids need you, there's a trip coming up, the clinic is closed on Sunday — every reason is reasonable. But many patients look back and say the same thing: if I'd had it checked a few days earlier, it wouldn't have become this complicated.
Relying on painkillers indefinitely
Painkillers can ease pain temporarily. But if you need more and more, and they work for shorter and shorter periods, the thing to pay attention to is usually not the painkiller — it's the cause of the pain.
Matching yourself to photos and videos online
The same swollen gum, toothache or abscess can reflect entirely different diseases. Online images help you understand the general picture; they are not a basis for diagnosis.
Assuming "not that painful" means "not a problem"
Many dental diseases are not constantly painful. Some infections come and go; some problems produce no symptoms at all in the early stages. No pain does not mean no disease.
Avoiding the check-up because you fear the answer
For many people, the real fear isn't the dentist — it's hearing "extraction" or "root canal". Yet plenty of patients discover, after the examination, that the situation is not nearly as bad as they had imagined.
A Final Word
The hardest part of a dental emergency is often not the treatment — it's the information. When the pain is real, every article sounds plausible, every friend has a different story, and every forum offers a different answer. The harder you look for one certain answer, the more confusing it gets.
We hope this article has cleared up the most common misunderstandings. Toothache is a symptom, not a diagnosis. Painkillers relieve pain but don't fix the tooth. Pain that disappears is not the same as a tooth that has healed.
Most toothaches need a dentist's assessment; difficulty breathing or swallowing, severe infection or major trauma belong immediately in a hospital A&E. Government dental street sessions, hospital A&E and private dental care each have a distinct role — understanding what each covers helps you choose well when it truly matters.
We hope you read this today purely out of interest, not because you're in pain. But if one day you or your family faces a real dental emergency, we hope what you've read leaves you less anxious, less uncertain, and confident about your next step.


